 Cause and Effect Diagram is also known as Ishikawa Diagram or Fishbone Diagram. This tool helps your team to work through the possible underlying contributing factors of a problem and sort the factors into a few categories. The analysis enables your team to create insights into the problem and start to consider possible improvements or solutions.
Cause and Effect Diagram is also known as Ishikawa Diagram or Fishbone Diagram. This tool helps your team to work through the possible underlying contributing factors of a problem and sort the factors into a few categories. The analysis enables your team to create insights into the problem and start to consider possible improvements or solutions.
Fishbone Diagram is a commonly used Root Cause Analysis (RCA) tool to determine why a particular problem is occurring. It helps you to identify a wide range of possible contributing factors – not just the obvious most.
This tool graphically displays the relationship of the causes to the effect or outcome. It can also be used in identifying areas for improvement.
Causes are typically grouped under 6 categories, namely Manpower, Methods, Materials, Machine, Measurement and Mother Nature. The London Protocol identifies 7 categories of contributing factors, namely Patient Factor, Individual/Staff Factor, Team Factor, Work & Care Environment Factor, Organizational Factor, Task & Technology Factor, and External Factor.
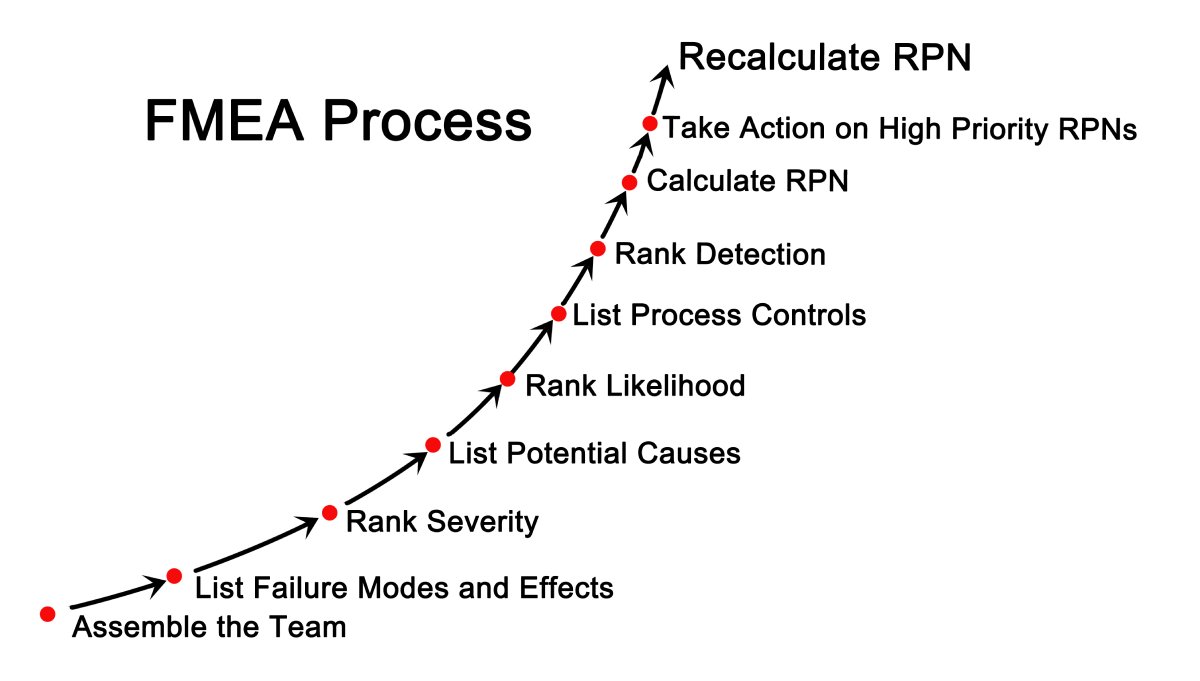 FMEA is a technique for conducting a systematic analysis of processes or products to identify and prevent any problems before they occur. It prompts your team to proactively review and evaluate what could go wrong (failure mode), why failures happen (failure causes), and the consequence of failure (failure effect). Improvement plans can then be carried out to prevent those failures.
FMEA is a technique for conducting a systematic analysis of processes or products to identify and prevent any problems before they occur. It prompts your team to proactively review and evaluate what could go wrong (failure mode), why failures happen (failure causes), and the consequence of failure (failure effect). Improvement plans can then be carried out to prevent those failures.
The focus of FMEA is to proactively identify potential risks or failure points and their impact, prevent failures and make the system more resilient. The emphasis is on preventing or reducing harm to patients or staff. FMEA is particularly useful in evaluating a new process prior to its implementation, and in assessing and managing the impact of the proposed change to existing processes. Healthcare organizations should apply FMEA to access new services and procedures before implementing them.
In an FMEA exercise, the team comprising representatives from all areas of the process under review convenes to discuss and predict where, how, and to what extent the system might fail. Failure mode with high Risk Profile Number (RPN) are probably the most important parts of the process on which to focus improvement efforts. Team members will then prioritize and work together to devise improvement plans to prevent those failures — especially failures that are likely to occur or would cause severe harm to patients or staff.
 The Pareto principle, commonly known as the “20/80 rule”, is an important quality tool for safety and process improvement. According to the Pareto principle”, in any group of factors that contribute to an overall effect, roughly 80% of the effect comes from 20% of the causes.
The Pareto principle, commonly known as the “20/80 rule”, is an important quality tool for safety and process improvement. According to the Pareto principle”, in any group of factors that contribute to an overall effect, roughly 80% of the effect comes from 20% of the causes.
Using a Pareto chart helps your team to prioritize and focus on patient safety interventions that have the greatest impact, thus saving effort and costs. This tool enables the team to make informed decisions and concentrate on the “vital few” (the factors that have the largest contribution to the effect). It also provides a rationale for not taking actions on the “useful many” (factors that have a relatively smaller contribution to the effect).
A Pareto chart is mainly used in the phase of problem identification. It presents the data in a visual manner and helps your team to communicate the problem or situation to senior management and seek their support or actions. Pareto chart is in a bar chart format in which the various factors that contribute to an overall effect are arranged in order from the largest to the smallest contribution to the effect.





